by McCollum Consultants
What is the prostate?
The prostate is a walnut-sized gland found in the male reproductive system which secretes enzymes into the semen to maintain its fluid state, thus allowing optimum transport of sperm.
The prostate can be divided into three different zones:
- Central zone: cells surrounding the ejaculatory ducts;
- Transitional zone: cells lying centrally and surrounding the urethra;
- Peripheral zone: cells comprising the main body of the gland.
Where is the prostate?
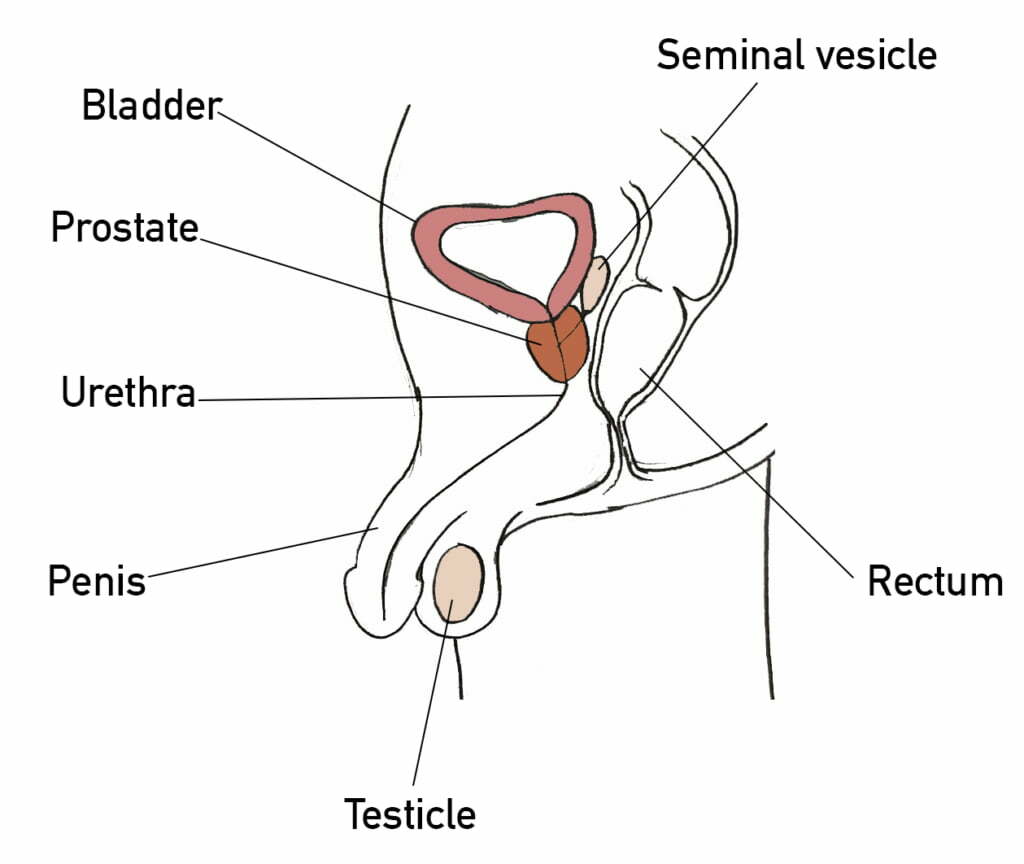
The prostate lies behind the neck of the bladder, above the external urethral sphincter, and in front of the rectum. The urethra runs from the bladder, through the prostate, and into the penis.
What is Benign Prostatic Hyperplasia (BPH)?
With age, the prostate naturally becomes larger due to proliferation of cells (hyperplasia) in the transitional zone. Often, this enlargement is completely benign and known as benign prostatic hyperplasia (BPH). The enlarged prostate can compress the urethra, and therefore classically presents with the following symptoms, which reflect impaired storage of urine and impaired voiding of urine:
- Nocturia (needing to urinate at night)
- Urinary frequency
- Urinary urgency
- Poor urine stream or an intermittent urine stream
- Difficult to initiate urination
- Terminal dribbling (dribbling of urine after urination)
Whilst completely benign, BPH can cause significant problems for individuals and can even lead to urinary tract infections (UTIs), urinary retention, and kidney damage.
Treatments available include:
- Lifestyle modifications
- Bladder training
- Catheterisation
- Medications
- Surgery
Medical treatments include:
- Alpha-blockers – relax muscles making it easier to pass urine.
- Anticholinergics – relax the bladder muscle.
- 5-alpha reductase inhibitors – shrink the prostate.
- Diuretics – increase the rate of urine production, therefore when taken during the day, it can reduce the amount of urine produced at night and reduce nocturia.
- Desmopressins – slow the rate of urine production, therefore when taken at night, they can reduce nocturia.
Surgical treatments include:
- Transurethral resection of prostate (TURP) – removal of part of the prostate.
- Prostatectomy – removal of the entire prostate.
- Prostatic urethral lift (PUL) implant – inserted to lift the prostate away from the urethra.
- Cystoplasty – surgery to increase the size of the bladder.
- Prostate artery embolisation – blocking the artery that supplies the prostate leads to the prostate shrinking in size.
- Botox injection of the bladder – to reduce oversensitivity of the bladder.
- Implanted sacral nerve root stimulation – signals sent stimulate pelvic floor contraction, building their strength over time.
- Urinary diversion – the ureters are disconnected from the bladder and redirected through a stoma.
- Water ablation – water is injected into the prostate causing pressure to destroy the prostate tissue.
- Rezum – Steam ablation
What is prostate cancer?
Prostate carcinoma is the most commonly diagnosed cancer in men. Some forms of prostate cancer are so slow growing that they do not present with symptoms, nor do they affect how long the person will live. However, some forms of prostate cancer are rapidly growing, will spread throughout the body, and cause symptoms and require treatment.
There are four main types of prostate cancer:
- Acinar/Ductal adenocarcinoma of the prostate: the most common type of prostate carcinoma.
- Transitional cell carcinoma of the prostate: usually starting in the bladder and spreading to the prostate.
- Squamous cell carcinoma of the prostate: grow and spread quite rapidly.
- Small cell prostate cancer: the fastest growing and spreading.
How is prostate cancer diagnosed?
The Physician will perform a digital rectal exam (DRE), whereby a gloved finger is placed into the rectum to examine the prostate. It is important to note that only one surface of the prostate is palpable via DRE. A normal prostate usually feels smooth and soft. An abnormal prostate may feel hard or nodular, or excessively large.
A blood test will be performed to measure the PSA level (see below).
A multiparametric MRI scan (mpMRI) may be performed to produce a more detailed image of the prostate. This helps the specialist to decide if a biopsy is necessary, where the biopsy should be taken from, and to observe the surrounding structures for any abnormalities and signs of a cancer spreading. Once the imaging has been performed, a Likert or PI-RAD score will be produced to indicate how likely the person is to have prostate cancer.
A biopsy of the prostate may be taken via:
- Transrectal ultrasound scan (TRUS) guided biopsy
- Transperineal biopsy
What is Prostate Specific Antigen (PSA)?
PSA is a protein produced by both normal and cancerous prostate cells. Significantly elevated numbers can indicate prostate cancer, however it may also indicate prostatitis (inflamed prostate) or a urinary tract infection (UTI). The PSA level also slightly increases with age.
How is prostate cancer graded and staged?
Prostate cancer is staged using the TNM system:
Tumour – size
Node – lymph node involvement
Metastasis – spread to other areas of the body
The Gleason score grades prostate cancer by assessing how aggressive and likely they are to spread the cancer cells are.
The Cambridge Prognostic Group (CPG) tool uses PSA level, TNM staging, and Gleason score to categorise prostate cancer into different risk groups.
It is important to grade and stage prostate cancer as this provides a prognosis and direction for treatment.
Prostate cancer can also be defined as the following:
- Localised i.e., it is contained within the prostate gland.
- Locally advanced i.e., it has just breached the prostate capsule.
- Advanced i.e., it has spread to other parts of the body. This may also be referred to as metastatic prostate cancer.
How can prostate cancer be treated?
Many people with prostate cancer will not require active treatment, and may be managed with active surveillance. This is often the case for those with localised, low grade prostate cancer.
Localised, low grade prostate cancer treatments include:
- Active surveillance
- Watch and wait
- Radical prostatectomy
- External beam radiotherapy
- Brachytherapy – radioactive seeds are placed into the prostate and deliver a steady rate of radiotherapy over several months.
- High-intensity focal ultrasound (HIFU)
- Cryotherapy
Locally advanced prostate cancer treatments include:
- External beam therapy with hormone therapy
- Brachytherapy
- Hormone therapy alone – reduces the production of testosterone, or inhibits testosterone from having an effect on cancer cells.
- Radical prostatectomy
- Radiotherapy
- High-dose rate brachytherapy
Advanced prostate cancer treatments do not aim to cure the cancer, rather the treatments hopefully keep it under control and manage symptoms. Treatments include:
- Chemotherapy with hormone therapy
- Hormone therapy alone
- Radium-223
- Various clinical trials
What are the complications of the treatment of prostate cancer?
As with all medical and surgical intervention, the treatment of prostate cancer carries the risk of complications and side effects. The side effects generally include:
- Erectile dysfunction
- Urinary incontinence
- Bowel dysfunction
- Infertility
Hormone therapy can also produce additional side effects that are linked to the reduced levels of testosterone. Not all side effects may be experienced, however they include:
- Hot flushes
- Fatigue
- Reduced libido
- Erectile dysfunction
- Orgasm dysfunction
- Change in size and shape of penis and testicles
- Weight gain
- Loss of strength and muscle mass
- Poor memory
- Reduced concentration
- Gynaecomastia – swelling and tenderness of the breast tissue
- Reduced body hair
- Osteopenia
- Mood disturbance