by Mr Graham Young, Consultant Urological Surgeon & expert witness
What is a urine infection? How do they vary?
A urinary tract infection (UTI) is an infection in any part of the urinary system—the kidneys, bladder, ureters, urethra, as well as the prostate in men. The most common cause of these infections is from bacteria that originate from the bowel and are present on the skin and around the urethra-bacteria usually enter the urinary system via this route.
Urinary tract infections vary enormously in their clinical significance; they can be anything from a mild cystitis that resolves itself, to infections causing sepsis that may be life-threatening. The latter, more serious type tend to be those that involve the kidneys (called pyelonephritis or pyonephrosis). These require very timely recognition and treatment. Failure to recognise such serious infections or manage them correctly can lead to prolonged morbidity, short or long-term organ damage and even mortality. It is therefore important for clinicians to have a high index of suspicion for such infections and know how to treat them.
How do clinicians recognise urine infections & what are the pitfalls?
Urine infections may begin with subtle symptoms and signs. Classically, infections of the lower part of the urinary tract (mainly bladder infections) tend to cause symptoms such as burning when passing urine (dysuria), urinary urgency, and frequency. Infections of the upper part of the urinary tract, in particular kidney infections, in addition tend to cause symptoms such as fever, shivering, flank or back pain, nausea, and feeling systemically unwell. However, clinical presentation does vary widely in different patient groups. A common example of this is in older adults, where there may be an absence of fever, and the first signs may be confusion or a more general and non-specific functional decline (often labelled “off legs” on admission). Therefore, if presentation is with non-specific symptoms, clinicians may incorrectly attribute other causes to a patient’s deterioration or may be late in recognising the seriousness of the infection.
Symptom patterns are also often atypical in immunosuppressed patients, whose body may not produce the usual inflammatory/immune reactions that normally results in the typical symptoms described above. Such patients are increasingly common and include patients on steroids, organ transplant patients and those on monoclonal antibody therapies. In addition, diabetes, spinal cord injury and pregnancy may also increase the risk that infections can ascend to the kidneys and reduce the ability of the immune system to counter such infections. This may cause a particularly rapid deterioration from an apparently mild infection to one that becomes life-threatening.
What tests are available to clinicians to help with diagnosis and what are the problems with these?
When a patient presents to General Practice or a Hospital Emergency Department, urine dipstick testing is the usual initial investigation. This consists of exposing a patient’s urine sample to a test strip. This has colorimetric tests for the presence of a variety of chemicals and enzymes within the urine that are either produced by bacteria or the body’s response to infection (Figure 1).
Clinicians look in particular for the presence of nitrites (a metabolic product of bacteria) as well as leucocytes (white blood cells), which represent the body’s response to an infection. Whilst the presence of these is likely to indicate infection, absence does not always exclude it. Diagnostic investigations are therefore not always reliable, particularly in the initial period of an infection when time may be of the essence in terms of both correct diagnosis and rapidly initiating treatment.
Other problems that may occur include patients not being able to produce a urine sample, particularly if unwell and dehydrated. Increasing use of remote consultations and telemedicine can also make it more difficult to obtain appropriate urine samples to aid diagnosis. Incompletely treated infections are not uncommon and can occur when a patient has been prescribed an “incorrect” antibiotic, due, for example to bacterial antibiotic resistance, or if a course of antibiotics is too short. This can produce a false negative on a dipstick test or even on a full laboratory urinalysis and culture.
A mid-stream urine sample sent to the microbiology laboratory for microscopy and culture analysis is the gold standard investigation for urine infections. If bacteria are found to be present, the sample is grown and screened against a variety of antibiotics to assess the best choice and if antibiotic resistance is present. However, this full result takes 3 or more days typically, during which time clinicians are forced to choose an antibiotic on a blind empirical ‘best guess’ depending on what they feel is the likely source of infection. Accuracy of this testing also relies on a sample being promptly received and processed by the laboratory (delays can result in bacteria not surviving within the sample and therefore not being detected).
What are the challenges in how clinicians should initially treat urine infections?
The commonest bacterial pathogens in urine (Escherichia coli, Klebsiella and Enterococcus faecalis) tend to have different antibiotic sensitivities, and even assuming that a urine culture can be obtained and processed properly, it will be several days before a clinician will have a laboratory report to inform them of the optimal antibiotic choice. Before this, “best guess” on antibiotic choice is made on the basis of, firstly, any previous urinalysis reports and, secondly, in conjunction with local Primary or Secondary Care guidelines on the treatment of UTIs. It is important for clinicians to liaise regularly with their local microbiology service and to be thoroughly familiar with prescribing guidelines, due to the increasing prevalence of antimicrobial resistance and how patterns of resistance change over time.
Whilst waiting for the full laboratory report, infections have the potential to progress or be incompletely treated, if the antibiotic initially chosen turns out not to be optimal. Furthermore, ineffective initial therapy may allow bacterial proliferation and selection of multidrug‑resistant strains. Subsequent infections become harder to treat, require broader‑spectrum or intravenous agents, and can lengthen hospital stay and increase costs and adverse effects both to the individual patient and the healthcare system.
At the individual level, adverse drug reactions are also not trivial nor infrequent; fluoroquinolones can cause tendinopathy and rupture aminoglycosides can be nephrotoxic or impair hearing; sulfonamides can provoke severe allergic reactions. Incorrect antibiotic choices can therefore expose patients to these risks without corresponding benefits.
Incorrect treatment can also result from insufficient duration of antibiotic courses, either due to a GP prescribing a short course or a patient prematurely discontinuing antibiotics when they feel that their symptoms have settled. Antibiotic choice can also be restricted due to potential interactions with a patient’s other medications such as fluoroquinolones and antiepileptic medications. Clearly in pregnancy many antibiotics are also contraindicated due to the risks of foetal malformation.
Another potential area for misunderstanding and inappropriate management is in patients who have urinary catheters. Urine from patients with catheters is almost always colonised with skin bacteria and in itself this is not harmful. Over treating this with antibiotics can fuel resistance. On the other hand, under recognising catheter associated UTIs can risk sepsis. Removing or replacing the existing catheter is also often necessary; antibiotics alone may fail if biofilms of bacteria persist on the catheter.
Failure or delay in recognising the development of sepsis itself is a common medicolegal problem. The reasons for this failure are multiple; inexperience of resident doctors and non-specific patient symptoms are not uncommon. Other problems can occur on short-staffed wards where clinical observations of pulse, respiratory rate, temperature and blood pressure may not be performed as frequently as desirable leading to delays in recognising clinical deterioration in patients.
What are the risks of missing or mismanaging a serious UTI?
The risks of missing or mismanaging a serious UTI are significant; the most serious is the potential of progression to sepsis. Sepsis is a condition when the body mounts a systemic inflammatory reaction in its efforts to fight the cause of the infection. Unfortunately, the variety of chemical messengers and cells that the body releases can result in reduced blood flow to vital organs, leakage of fluid from blood vessels and secondary damage to organs. Untreated sepsis has a very high mortality.
As an example within urology, the kidneys’ function is commonly affected in sepsis of any cause, and in particular urinary tract sepsis. This can result in both acute loss of function, and if inadequately treated there may be long-term loss of function as well.
In pregnancy, failure to treat pyelonephritis promptly can harm both mother and baby. Pyelonephritis can be associated with complications including sepsis and preterm labour. This then endangers the fetus. Screening and prompt treatment of bacteriuria in pregnancy are essential.
Summary
UTIs are a very common cause of bacterial infection in humans and vary from the trivial to the fatal. Current technologies for diagnostics are imperfect and can result in initially incorrect antibiotic choices, exposing a patient to the risk of sepsis in particular.
Maintaining a high index of suspicion is important, particularly in high risk patient groups such as elderly, immunocompromised patients or in pregnancy. Clinicians need to be aware of atypical presentations such as confusion, falls or non-specific malaise.
In outpatient settings, patient should be reviewed at 48-72 hours to assess response, review results of laboratory microbiology tests, and if necessary change the antibiotic utilised. With more critically ill inpatients, observation should be close enough to pick up signs of deterioration rapidly so that treatment can be escalated if necessary even to an intensive care setting.
Figure 1 A urine dipstick
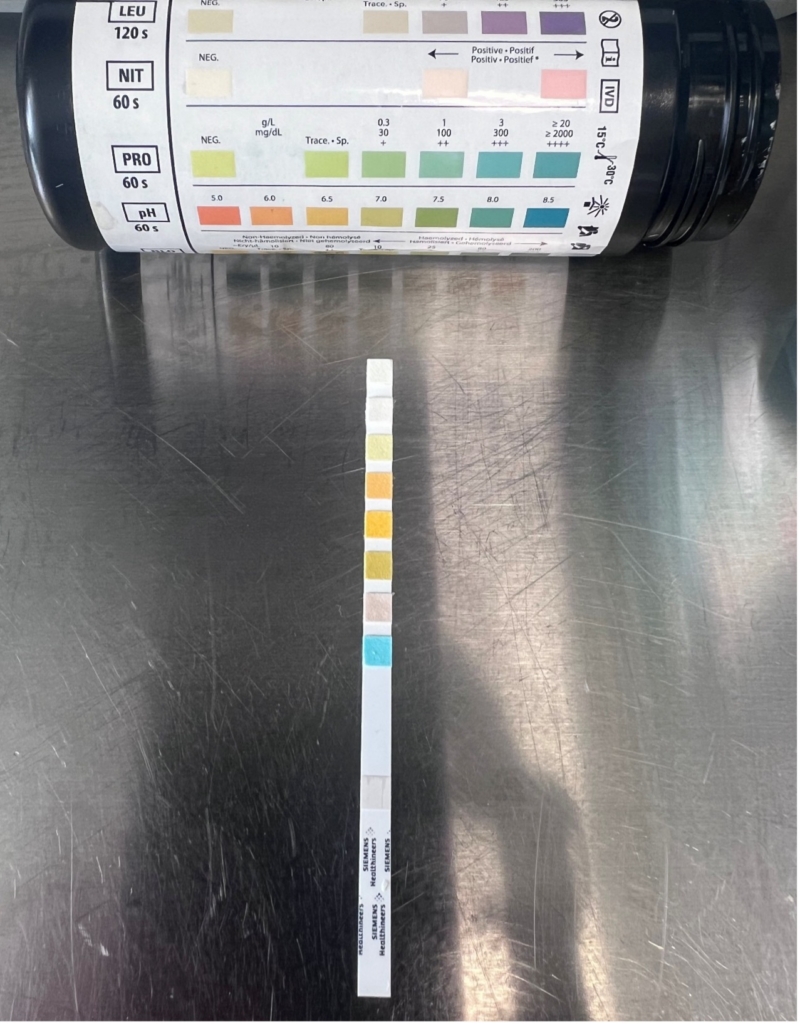
Figure 2: A typical laboratory urine culture report indicating growth of a bacterium (E Coli) and the most appropriate antibiotics choices
Culture :
>100 CFU x 10*6/L Escherichia coli Abnormal
Susceptibility
| Escherichia coli | |||
| ANTIBIOTIC SUSCEPTIBILITY | ANTIBIOTIC SUSCEPTIBILITY (DISC) | ||
| Amoxicillin | Resistant | ||
| Cefalexin | Resistant | ||
| Ciprofloxacin | Susceptible | ||
| Co-Amoxiclav | Resistant | ||
| Fosfomycin | Susceptible | ||
| Nitrofurantoin | Susceptible | ||
| Pivmecillinam | Susceptible | ||
| Trimethoprim | Resistant | ||